TYPE 1 DIABETES

Me: Siri, play “Lollipop” by The Chordettes.
Siri: Ok, now playing “Lollipop” from Apple Music.
Lollipop lollipop, Oh lolli lolli lolli, lollipop, lollipop, Oh lolli lolli lolli, lollipop, lollipop, Oh lolli lolli lolli, lollipop.

There is a BIG MYTH that eating sugar causes diabetes. I mean, if that were the case, then those with a sweet tooth like my dear sister H and aunt P would most certainly be diabetic. The truth of the matter is, eating sweets alone can not lead to diabetes, there have to be other conditions leading to the onset of the disease.

There are two types of diabetes, Type 1 and Type 2. For today we will discuss Type 1 diabetes.
What is diabetes?
Diabetes mellitus commonly known as diabetes refers to a group of diseases in which the body does not produce enough or respond normally to insulin, causing blood sugar (glucose) levels to be abnormally high. Insulin is a hormone that the body needs to manage blood glucose levels.
Type 1 diabetes formerly known as insulin-dependent diabetes or juvenile-onset diabetes, for reasons that are not clear, is when the body’s immune system attacks the insulin-producing cells (beta cells) of the pancreas, and more than 90% of them are permanently destroyed. Simply put, this means that your pancreas doesn’t make insulin or makes very little insulin. Without insulin, blood sugar (glucose) cannot enter cells and accumulates in the bloodstream causing hyperglycemia. High blood sugar is harmful to the body and is responsible for numerous diabetes symptoms and complications.
Type 1 diabetes affects only around 5 to 10% of people with diabetes, and it typically develops in children, adolescents, and young adults, but it can happen at any age.
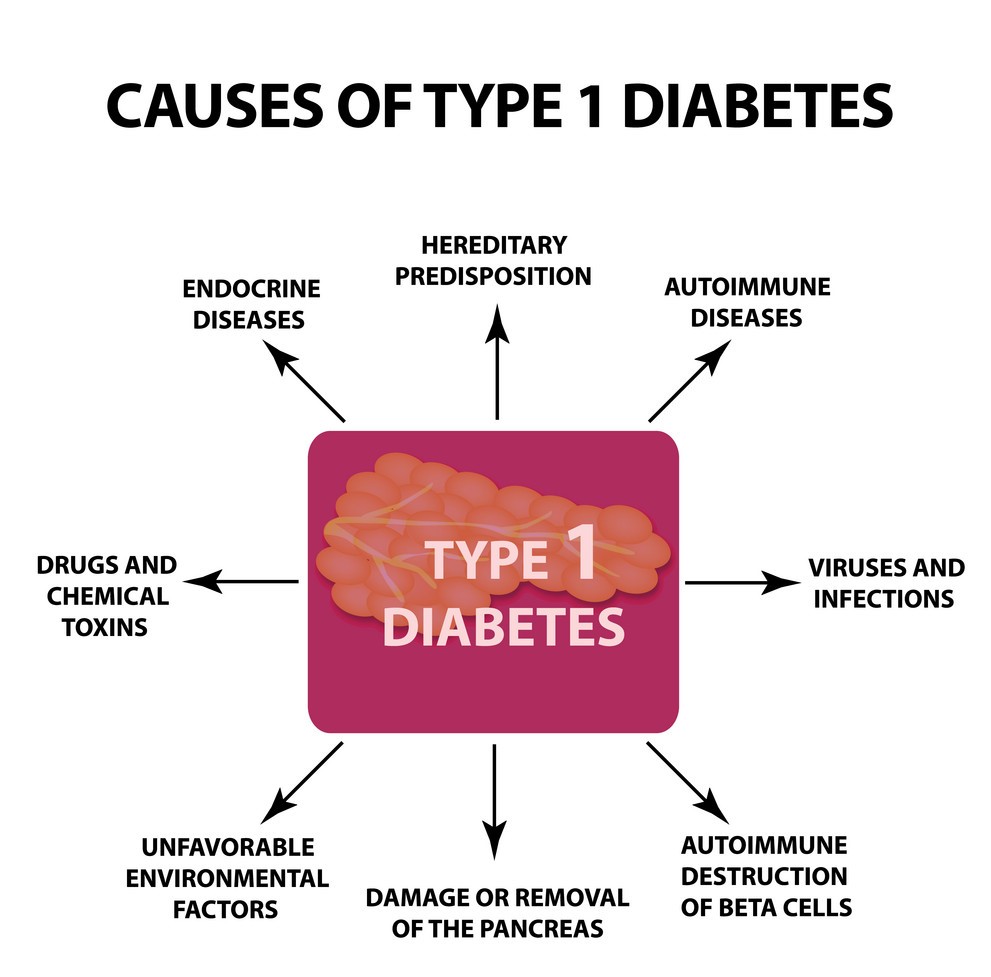
CAUSES
1. As I mentioned earlier, Type 1 diabetes is caused by the destruction of beta cells (β-cell), the only cells in the body that are capable of producing insulin. The best-studied components of this autoimmune response are antibodies that target beta cells and begin to grow months or years before the onset of symptoms. Typically, a person will produce antibodies against insulin or one of the main autoantigens in type 1 diabetes (protein GAD65) first. Protein GAD65 is a membrane‐bound enzyme on the pancreatic beta‐cells, glutamic acid decarboxylase 65. This is then followed by the production of antibodies against IA-2, IA-2 β, and/or ZNT8.
NB: IA-2 (insulinoma-associated protein-2) is an intracellular protein, widely expressed in the body, which has a negative regulatory role on the insulin-signaling pathway.
-IA-2β (an identifier of PTPRN2 (protein tyrosine phosphatase receptor type N2) is a major autoantigen associated with Type 1 diabetes.
-ZNT8 (zinc transporter 8) is an islet β-cell secretory granule membrane protein that was identified as an autoantibody antigen in type 1 diabetes.
People who have more of these antibodies and who develop them earlier in life are more likely to develop type 1 diabetes symptoms. It’s still not clear what causes these antibodies to develop.
2. Genetics: Some individuals have genes (partially inherited characteristics) that increase their risk of developing type 1 diabetes. Relatives of type 1 diabetics have an increased risk of inheriting the condition. A 1% to 9% greater risk exists for children of parents with Type 1 diabetes.
3. Environmental: Scientists believe that an environmental factor possibly a viral infection or a nutritional factor during childhood or early adulthood causes the immune system to destroy the insulin-producing cells of the pancreas. Numerous environmental and personal factors are connected with modest increases in type 1 diabetes risk, although the relationship between each risk and diabetes is sometimes unclear. Children whose mothers are obese, older than 35, or who were born via cesarean section have a slightly increased risk of developing type 1 diabetes. Similarly, a child’s weight gain in the first year of life, total weight, and body mass index (BMI) are connected with a marginally increased chance of developing type 1 diabetes. Also connected with type 1 diabetes risk is the consumption of cow’s milk and dietary sugar intake. Animal research and some large human studies have identified minimal connections between the incidence of type 1 diabetes and the consumption of gluten or dietary fiber; however, other large human studies have not found such an association.
4. Medications: Certain medications can inhibit insulin synthesis or damage beta cells, resulting in a disease resembling type 1 diabetes. The antiviral medication, Didanosine, promotes pancreas inflammation in 5 to 10% of persons who take it, sometimes causing persistent β-cell damage. Similarly, up to 5% of persons who use the anti-protozoal medication, Pentamidine, have β-cell damage and diabetes. Statins (which may also damage cells), the post-transplant immunosuppressants, Cyclosporin A, and Tacrolimus, the leukemia medication, L-asparaginase, and the antibiotic, Gatifloxacin, all-cause diabetes by reversibly reducing insulin secretion. Opdivo among other Cancer Immunotherapy drugs has also killed pancreatic beta cells.
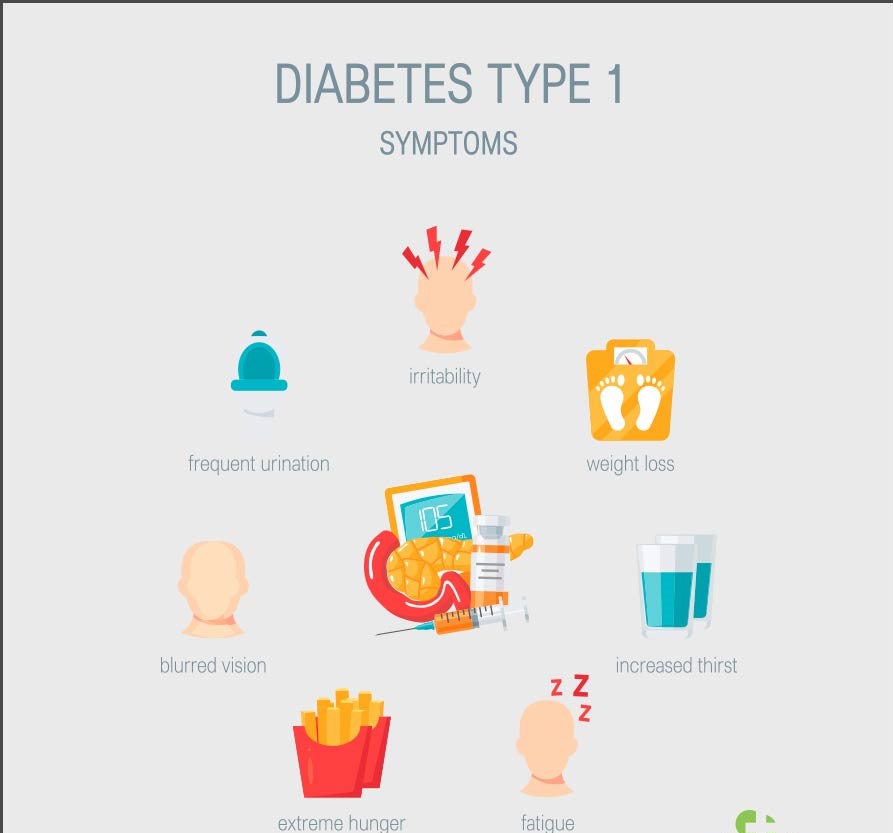
SYMPTOMS
The symptoms of type 1 diabetes often manifest within a few days to weeks. They consist of:
- increased hunger and thirst
- frequent urination
- blurred vision
- tiredness and fatigue
- weight loss without an apparent trigger or cause
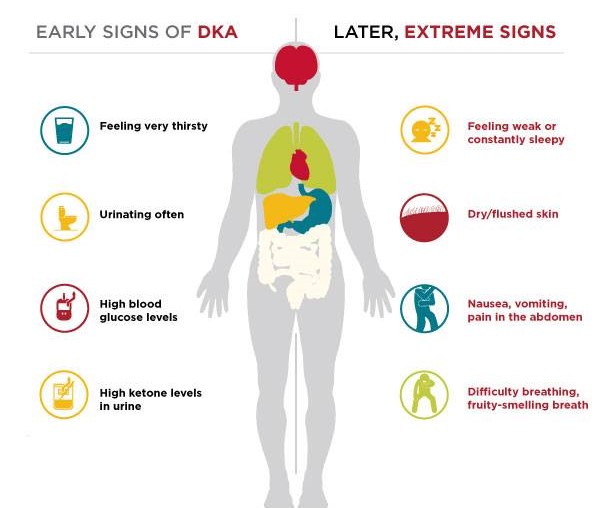
One in three children will exhibit the initial symptoms of diabetic ketoacidosis (DKA). This is a potentially fatal disorder in which excessive ketones circulate throughout the body, resulting in acidosis. It requires immediate medical care. Symptoms include:
- a fruity smell on the breath
- dry or flushed skin
- nausea or vomiting
- abdominal pain
- breathing difficulty
- confusion and difficulty focusing
Honeymoon phase
When a person is first diagnosed with diabetes, their body may continue producing insulin for some time. Throughout this period, their insulin levels may fluctuate. They may require fewer insulin injections to maintain appropriate blood glucose levels – this is known as the honeymoon phase.
As the individual adjusts their insulin dosage, their condition may appear to be improving. This however is unlikely to be the case. During this time, individuals should continue to collaborate with their healthcare team and adhere to the suggested treatment plan.
IS ALL TYPE 1 DIABETES THE SAME?
Accumulating evidence suggests that patients with type 1 diabetes who have a family history of the disease (defined as having at least one first-degree relative with type 1 diabetes) — often have a significantly different disease course than those with sporadic type 1 diabetes who have no family history.
The most notable difference is that familial cases are associated with a much greater number of comorbidities.
A recent report on more than 16,000 US residents with type 1 diabetes who were enrolled in a national registry revealed that among the 3,941 adults and children with a familial background, various comorbidities were much more prevalent than among the more than 12,000 patients with sporadic type 1 diabetes, which was defined conservatively as not having any relatives who had been diagnosed with it, including those more than first-degree removed.
Those with the familial disease had considerably higher prevalence rates of hypertension, hyperlipidemia, atherosclerosis, retinopathy/maculopathy/vitreopathy, erectile and sexual dysfunction, gastroesophageal reflux disease, neuropathy, and nephropathy, as well as rates of various other comorbidities. People with sporadic cases of type 1 diabetes were substantially more likely to be asymptomatic. Several comorbidities among familial individuals in the investigated population clustered in groups of two or three. Using a custom-designed analytical data-mining method, the researchers discovered these prevalence trends.
DIAGNOSIS
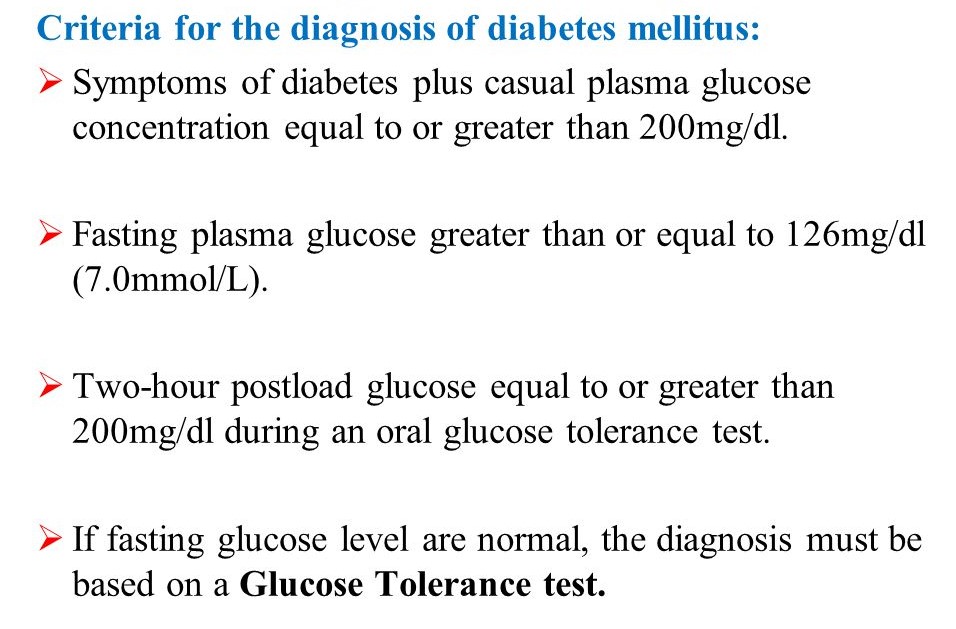
Diagnostic tests include:
- Glycated hemoglobin (A1C) test; This blood test determines your average blood sugar level over the last two to three months. It quantifies the quantity of blood sugar bound to the oxygen-carrying protein in red blood cells (hemoglobin). The higher your blood sugar levels, the more sugar-attached hemoglobin you’ll have. Diabetes is diagnosed when your A1C result is 6.5% or above on two different tests.
- Random blood sugar test; A blood sample will be drawn at random and validated by additional testing. The concentration of sugar in the blood is measured in milligrams per deciliter (mg/dL) or millimoles per liter (mmol/L). A random blood sugar level of 200 mg/dL (11.1 mmol/L) or higher, regardless of when you last ate, indicates diabetes.
- Fasting blood sugar test; After you do not eat (fast) overnight, a blood sample will be taken. A fasting blood sugar level of less than 100 mg/dL (5.6 mmol/L) is considered normal. Prediabetes is defined as fasting blood sugar levels ranging from 100 to 125 mg/dL (5.6 to 6.9 mmol/L). Diabetes is diagnosed when your blood sugar level is 126 mg/dL (7 mmol/L) or higher on two separate tests.
If you’ve been diagnosed with diabetes, your doctor may also order blood testing. These will look for autoantibodies, which are common in people with type 1 diabetes. When your doctor is unsure whether you have type 1 or type 2 diabetes, the testing can help. The presence of ketones — byproducts of fat metabolism — in your urine also indicates type 1 diabetes rather than type 2 diabetes.
TREATMENT
- Insulin is the primary treatment for type 1 diabetes. People can administer it in the following ways:
- a needle and syringe
- an insulin pen
- an insulin pump
Insulin comes in a variety of types, including;
- Short-acting insulin: This form of insulin, often known as regular insulin, begins to work roughly 30 minutes after injection. It reaches a peak effect at 90 to 120 minutes and has a duration of 4 to 6 hours. Humulin R, Novolin R, and Afrezza are a few examples.
- Rapid-acting insulin: This form of insulin begins to work within 15 minutes. It reaches a peak effect at 60 minutes and lasts approximately 4 hours. This is commonly used 15 to 20 minutes before meals. Glulisine (Apidra), Lispro (Humalog, Admelog, and Lyumjev), and Aspart (Novolog and FiAsp) are among examples.
- Intermediate-acting insulin: This form of insulin, also known as NPH insulin, begins to work in 1 to 3 hours. It reaches its peak effect at 6 to 8 hours and has a duration of 12 to 24 hours. Insulin NPH (Novolin N, Humulin N) is one example.
- Long- and ultra-long-acting insulin: This form of insulin may provide coverage for up to 14 to 40 hours. Examples include Glargine (Lantus, Toujeo Solostar, Basaglar), Detemir (Levemir), and Degludec (Tresiba).
A person diagnosed with Type 1 diabetes is most likely to require numerous daily injections of a combination of long-acting and rapid-acting insulin. These injections mimic the body’s regular insulin utilization more than prior insulin regimens that only required one or two doses each day. Three or more insulin injections per day have been shown to improve blood sugar levels.
If insulin does not completely regulate glucose levels, some patients may require extra medication, such as Pramlintide (Symlin), which helps manage glucose levels after eating.
2. Other medications: People with type 1 diabetes may also be prescribed other drugs, such as:
-High blood pressure medications: To maintain healthy kidneys, your doctor may give angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs). These drugs are advised for diabetics with blood pressures exceeding 140/90 millimeters of mercury (mm Hg).
-Aspirin: To protect your heart, your doctor may recommend taking baby or regular aspirin daily. Your doctor or nurse may believe that you are at a higher risk for a cardiovascular event. Your physician will address the risk of bleeding associated with aspirin use.
-Cholesterol-lowering drugs: Cholesterol recommendations are more stringent for diabetics due to their elevated risk of cardiovascular disease. Low-density lipoprotein (LDL, or “bad”) cholesterol should be less than 100 mg/dL (2.6 mmol/L), according to the American Diabetes Association. HDL, or “good” cholesterol, is recommended to be above 50 mg/dL (1.3 mmol/L) in women and greater than 40 mg/dL (1 mmol/L) in males. Another form of blood fat, triglycerides, should be fewer than 150 mg/dL (1.7 mmol/L).
3. Healthy eating: It is essential to base your diet on nutritious, low-fat, high-fiber foods like whole grains, vegetables and fruits. You’ll need to learn how to calculate the carbohydrate content of the meals you eat. You can give yourself enough insulin this way. This allows your body to appropriately utilize the carbohydrates. Your registered dietitian will advise you to limit your consumption of animal products and processed carbohydrates such as white bread and sweets. Even people who do not have diabetes should follow this healthy eating regimen. A trained dietician can assist you in developing a food plan that meets your specific requirements.

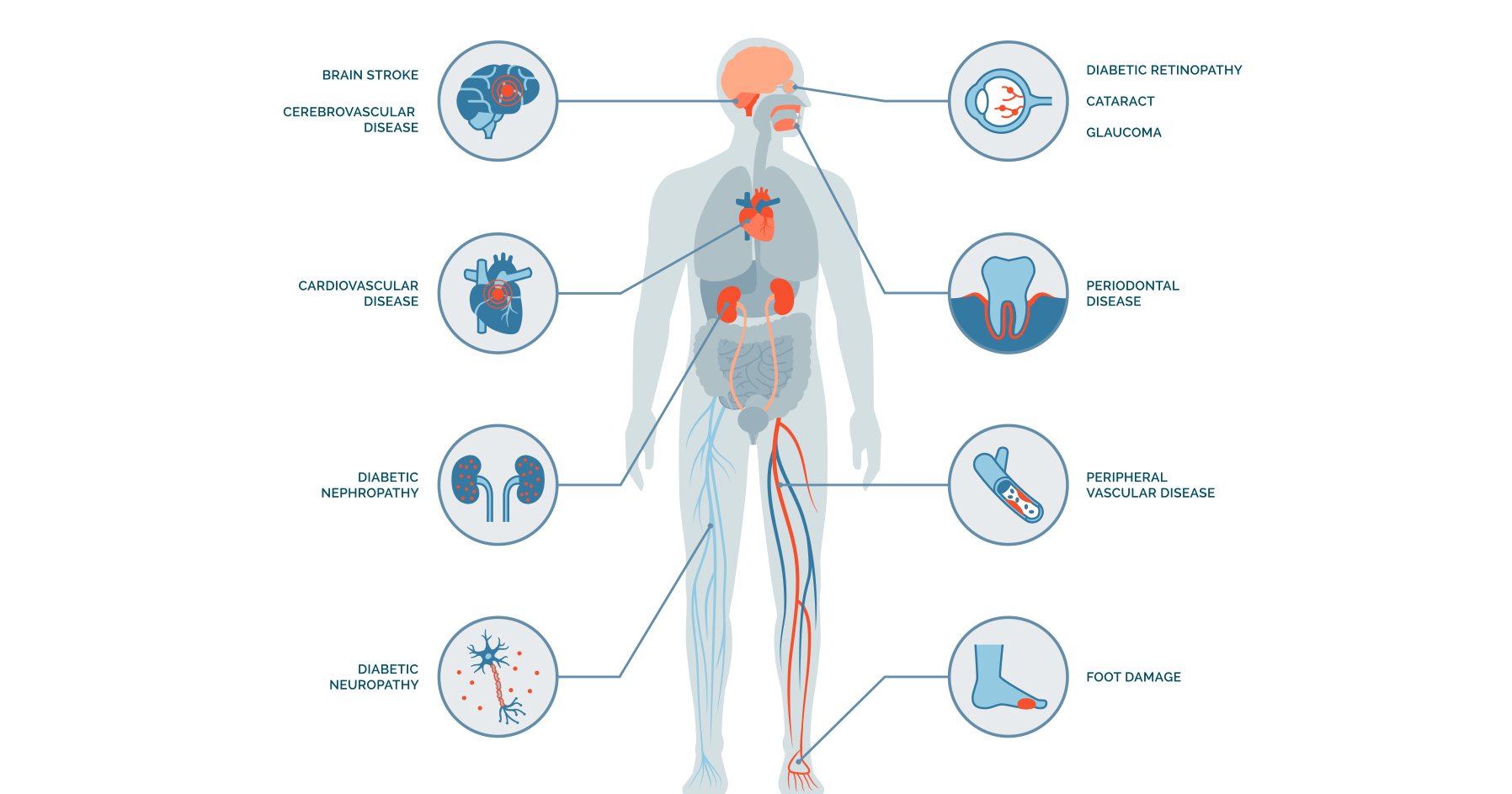
COMPLICATIONS
From head to toe, type 1 diabetes can cause a number of complications, such as stroke, blindness, amputation, and more. The stress of controlling their diabetes puts people who have it at risk for mental health problems including anxiety or depression. It is frequently called diabetes distress.
- Hypoglycemia (low blood sugar): This is one of the 2 most common complications of diabetes. Too much insulin, waiting too long for a meal or snack, not eating enough, and engaging in excessive physical activity are the most common causes. Hypoglycemia needs to be treated quickly.
- Diabetes ketoacidosis (DKA): This is the second most common complication of diabetes, DKA is a life-threatening complication of diabetes that can occur at any stage. DKA arises when there is insufficient insulin to allow glucose into the cells. DKA is caused by extremely high blood sugar and low insulin levels. Illness and skipping insulin injections are the most common causes. Consult your doctor and ensure that you understand how to prevent and treat DKA.
- Celiac disease: Celiac disease is a digestive disorder that appears to be more prevalent in type 1 diabetes patients than in the general population. Gluten, a protein present in wheat, rye, barley, and triticale, is intolerable to celiac patients.
- Nephropathy (kidney disease): Diabetes is associated with kidney disease, also known as nephropathy. If the kidneys are damaged as a result of high blood glucose (sugar) levels and high blood pressure, they will no longer be able to filter blood properly and may fail entirely. Kidney failure is a major complication of diabetes.
- Diabetic retinopathy (eye damage): Many patients with diabetes have “diabetic retinopathy,” which is eye damage. Diabetic retinopathy can result in vision loss or blindness. Blood sugar control, regular eye exams, and early treatment can reduce the likelihood or progression of eye damage.
- Heart disease & stroke: Diabetes increases your risk of heart disease and stroke. Diabetes can cause heart disease 15 years earlier than non-diabetics. Coronary artery disease is the most frequent type of heart disease in people with diabetes.
- Hypertension: Diabetes patients are far more prone than non-diabetics to develop heart disease and/or have a stroke at a younger age. Diabetes, combined with high blood pressure (commonly known as hypertension), places additional strain on your body. This can harm your heart, brain, kidneys, and eyes.
- Mental health issues: Many diabetics experience stress, lowered mood, and incapacitating levels of anxiety. Mental health issues can impair your capacity to manage and care for your diabetes. It is equally crucial to care for your mental health as it is for your physical health.
- Diabetic peripheral neuropathy: One of the long-term complications of diabetes is nerve damage, often known as diabetic peripheral neuropathy. If neglected, the damage produced by neuropathy can lead to infection and limb amputation.
Phewwwwwwww, that’s enough for today! With Valentine’s Day just a few weeks away, my parting gift to you is this sweet message below……
See you next time when we talk about Type 2 Diabetes!!