

We are living in an era where nothing seems to be going according to plan, what we envisioned life to be isn’t really how it’s turning out to be. From Covid-19 to wars to inflation to monkeypox to suicides, the list is like that song which goes, “this is the song that doesn’t end, yes, it goes on and on, my friends, some people started singing it not knowing what it was, and they’ll continue singing it forever just because,” then the song repeats itself endlessly. This will eventually be me if I commit myself to listing each and every barbarity that is currently on-going. Given all that’s going on, a lot of people are suffering mentally and maybe three-quarters don’t even realize that the current global situations are taking a toll on their mental health.

We have all had our fair share of misfortune in this lifetime. I mean, what would life be without the constant ups and downs, even the bible in Ecclesiastes 3 verses 1-8 mentions that “There is a time for everything and a season for every activity under the heavens”. During my first ever Philosophy lesson back in university, my professor’s opening remark was, “my friends, life is suffering”; the whole class burst into laughter, but, the older I get, I see that indeed, life is suffering, and all this suffering can lead one into a state of DEPRESSION.
What then is depression? The best definition I could come up with is this, depression is a mood disorder characterized by a pervasive sense of melancholy (sadness) and loss of interest. Depression, sometimes known as major depressive disorder (MDD) or clinical depression, affects how a person feels, thinks, and behaves, and can lead to a number of emotional and physical difficulties. One may have difficulty performing typical day-to-day tasks, and may occasionally feel that life is not worth living.
I am a Game of Thrones fanatic, matter of fact, that’s an understatement, I am obsessed with this series. My handle is even that of the great mother of dragons herself, the one, the only Khaleesi. Game of Thrones introduced us to a character, Jaqen H’ghar, an alias assumed by one of the Faceless men of Braavos. The faceless men can shapeshift into a new appearance and to them, they believe that death is a merciful end to suffering. I might be reaching, but hear me out, doesn’t that sound like depression? Let me break- down my theory. People with depression have a talent for masking their illness. These people can be the life of the party, they can be the ones always wearing a smile on their faces, offering others help in time of need, and, are often the first ones willing to lend a shoulder to cry on. But, when they are all alone, in the silence of their homes, they are the ones crying themselves to sleep, taking different drugs and substances to feel numb, and in some situations, they are the ones taking their own lives. To me, this is shapeshifting, and, it reminds me of the faceless men of Braavos.
CAUSES:
Depression is a complicated illness. It can occur for a variety of reasons; however, no one knows the precise causes. Some individuals experience depression during severe medical illnesses such as cancer, dementia,etc. Others may experience depression in response to life changes such as relocation or the loss of a loved one. Still, others have a history of depression in their family. Those who do may suffer from depression and experience overwhelming feelings of melancholy and isolation for no apparent reason.
Numerous factors can raise the likelihood of developing depression, including the following:
i) Abuse: Later in life, physical, sexual, or emotional abuse can make a person more susceptible to depression.
ii) Age: Elderly individuals are more susceptible to depression. This can be exacerbated by additional variables, such as living alone, regrets of failed expectations, and lacking social support.
iii) Certain medications: Medications, including isotretinoin (used to treat acne), interferon-alpha, and corticosteroids, can raise the risk of depression.
iv) Conflict: Personal conflicts or disagreements with family members or friends may trigger depression in a person who is genetically susceptible to it.
v) Loss: Sadness or grief following the death or loss of a loved one might increase the risk of depression.
vi) Gender: Women are more susceptible to suffering from depression than men. No one knows the reason why. The hormonal fluctuations that women experience throughout their lifetimes are most likely to play an impact.
vii) Genes: A history of depression in the family may raise the risk. It is believed that depression is a complex trait, meaning that rather than a single gene contributing to disease risk, there are likely several separate genes that individually exhibit tiny effects. The genetics of depression, like those of the vast majority of mental disorders, are not as basic or easy as those of purely hereditary diseases such as Huntington’s chorea or cystic fibrosis.
viii) Major events: Positive events such as starting a new career, graduating from college, or getting married might result in depression. Negative events too such as; moving, losing a job or income, divorcing, or retiring can also be life-altering.
ix) Social isolation: Exclusion from family or social groups and other mental illnesses may increase the likelihood of developing severe depression.
x) Serious illnesses: Depression may occur alongside serious illness or be precipitated by other medical conditions.
xi) Substance abuse: Nearly 45% of substance abusers suffer from significant or clinical depression. Although drugs or alcohol momentarily improve one’s mood, they will ultimately exacerbate one’s melancholy.
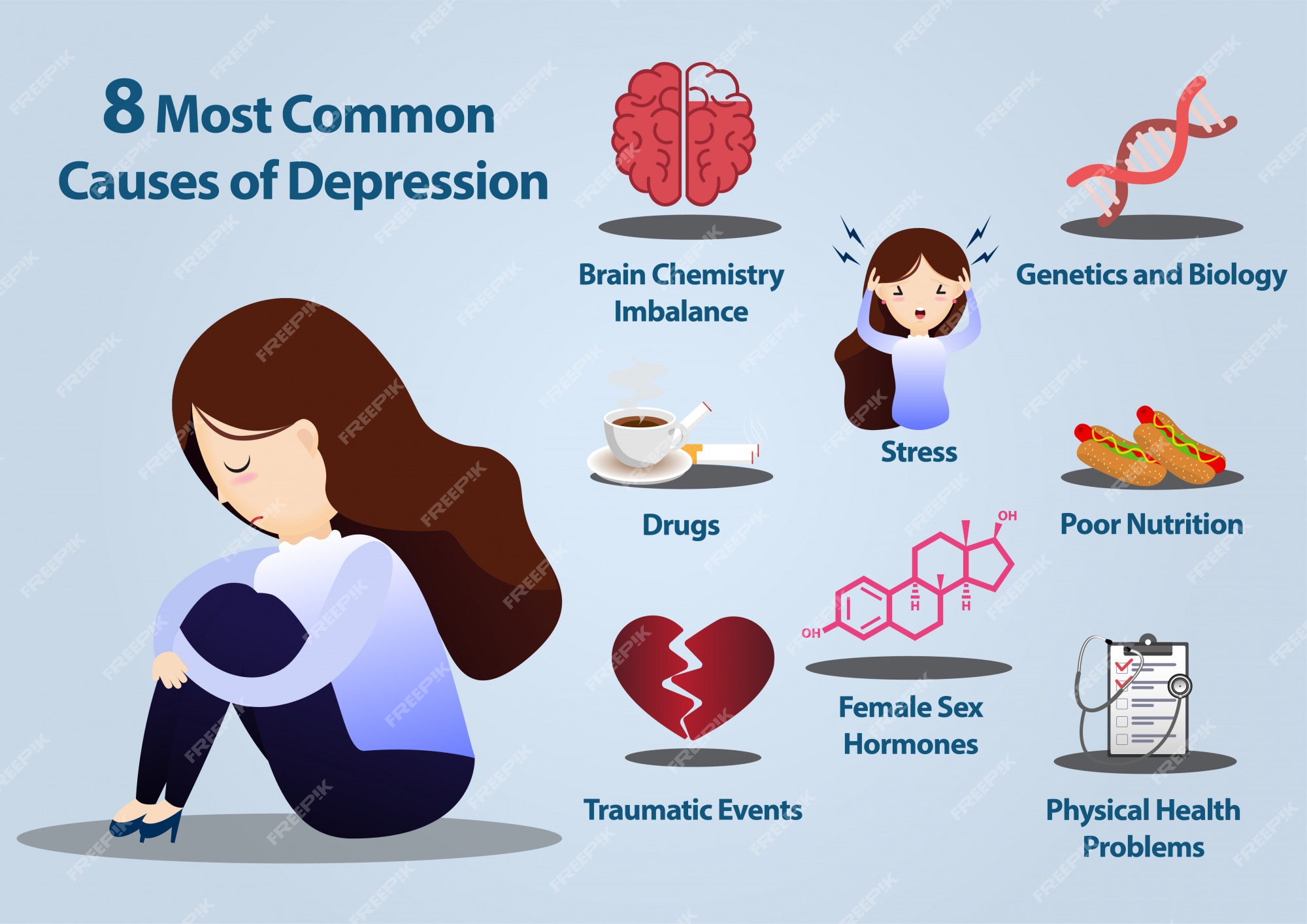
Biology and Depression:
A comparison done by researchers has shown abnormalities between the brains of those with clinical depression and those without. For instance, the hippocampus, (a small part of the brain that is essential for memory storage), appears to be smaller in some individuals with a history of depression compared to those who have never experienced depression. A smaller hippocampus contains fewer serotonin receptors. Serotonin is one of many brain chemicals known as neurotransmitters that enable communication between regions of the brain involved in emotion processing.
Scientists are yet to establish why certain depressed individuals have a smaller hippocampus. It has been discovered that depressed individuals create an excessive amount of the stress hormone cortisol. It is believed that cortisol has a harmful or “shrinking” effect on hippocampal formation.
Family history and Depression:
We are aware that depression may occasionally run in families. This shows that depression has at least a partial hereditary component. Children, siblings, and parents of individuals with severe depression are more likely to suffer depression than others. Multiple genes interacting with one another in unique ways are likely to contribute to the various inherited forms of depression. Despite the evidence of a familial link to depression, it is doubtful that there is a single “depression” gene, but rather a large number of genes that interact with the environment to produce minor impacts on depression.
SYMPTOMS:
There are numerous symptoms of depression, however, you may not exhibit them all. The intensity and duration of these symptoms vary from person to person.
Some of the many emotions you might experience include:
i) Depressed, void, or apprehended: These persist throughout time without improving or disappearing.
ii) Helplessness, worthlessness, or guiltiness: Preoccupation with losses and failures may have negative effects on oneself
iii) Hopeless: One may be gloomy and assume nothing positive will ever occur., to the point of one considering suicide.
iv) Irritable: You may get more agitated or irritable than normal.
v) Less enthusiasm for activities: Typically, enjoyable past-times,games, food, and/ or sexual desire may not appeal anymore.
vi) Less energetic: Daily routines and responsibilities may appear insurmountable. One may experience excessive fatigue and slower thinking.
vii) Difficulty concentrating: Focusing, reading, or watching television may become difficult. A person may have difficulties remembering specifics. It may appear daunting to make a decision, whether large or small.
viii) Changes in your sleeping habits: This is characterized by difficulties in falling asleep at night (insomnia). The inverse is also possible, one may sleep significantly longer than usual during daytime (hypersomnia), or one may have an uncontrollable urge to sleep during daytime (Narcolepsy).
ix) Alterations in appetite: A person may eat excessively or not eat at all. Depression frequently causes weight gain or loss.
x) Pains and aches: One may experience headaches, cramps, upset stomach, or digestive issues.

Patterns:
Depending on the frequency and severity of symptoms, as well as the effects on the individual’s functioning, depressive episodes can be classified as mild, moderate, or severe.
Different patterns of mood disorders include the following:
i) single episode depressive disorder; the individual’s first and only episode
ii) recurrent depressive disorder; the individual has a history of at least two episodes
iii) bipolar depressive disorder; depressive episodes alternate with manic symptoms, such as euphoria or irritability, increased activity or energy, and other symptoms such as increased talkativeness, racing thoughts, elevated self-esteem, decreased desire for sleep, distractibility, and impulsive hazardous behaviour.
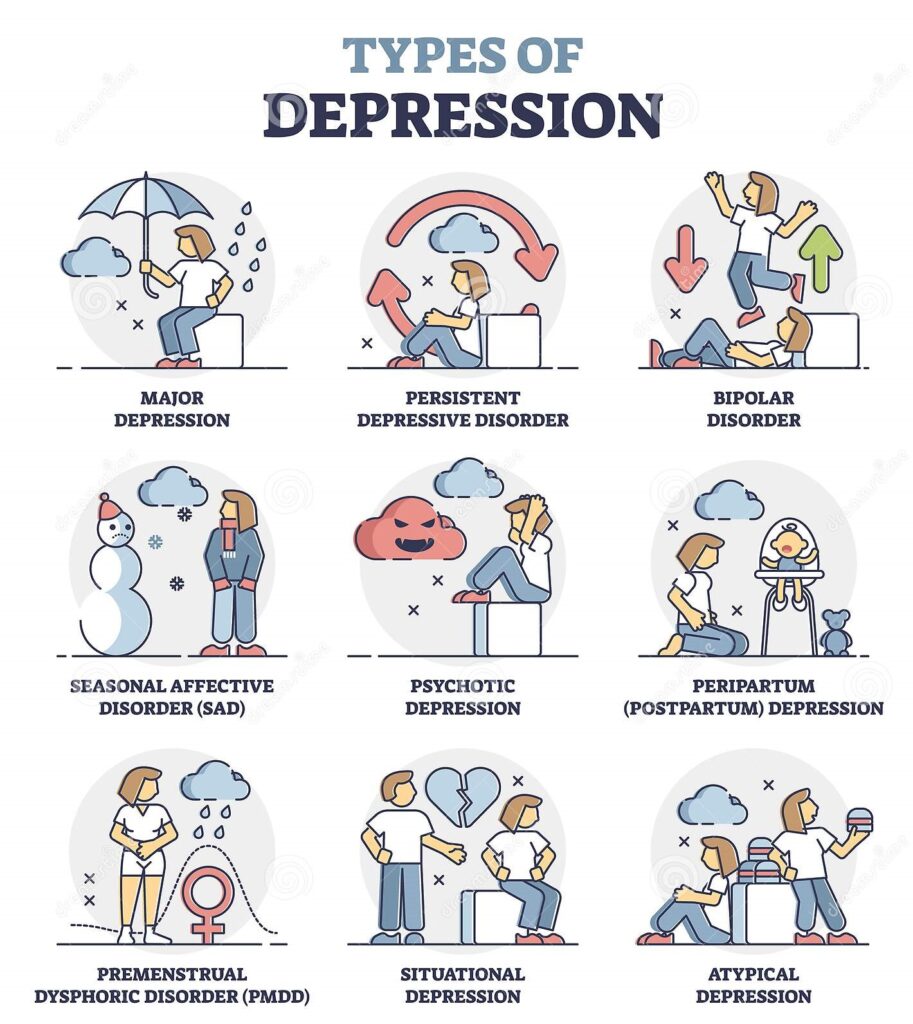
Types of Depression:
The four most prevalent kinds of depression are major depression, persistent depressive disorder, recurrent depressive disorder (formerly known as dysthymia), manic-depressive (bipolar) disorder, and seasonal affective disorder.
- Major depression: The classic depression type, major depression is characterized by an all-encompassing bad mood and a loss of interest in even typically joyful activities. This type of depression is characterized by difficulty sleeping, changes in food or weight, loss of energy, and a sense of worthlessness. There may be thoughts of death or suicide. Typically, it is treated with psychotherapy and medicines. Electroconvulsive therapy may be beneficial for some persons with severe depression that is not improved by psychotherapy or antidepressant drugs.
2. Persistent depressive disorder: Formerly known as “dysthymia,” this type of depression is characterized by a depressed mood that has persisted for at least two years but may not reach the severity of major depression. Many people with this type of depression are able to operate on a day-to-day basis but feel depressed or unhappy most of the time. Other signs of depression may include changes in eating and sleep, decreased energy, low self-esteem, and hopelessness.
3. Bipolar disorder: Bipolar disorder, formerly known as manic-depressive disease, is characterized by depressive episodes. However, they can experience periods of heightened energy or activity. Manic symptoms resemble the reverse of depressive symptoms: grandiose ideas, falsely high self-esteem, decreased need for sleep, faster thoughts and activity, and increased pursuits of pleasure, such as sex binges, overspending, and risk-taking. Mania can be enjoyable, but it is short-lived, can result in self-destructive conduct, and is typically followed by a period of sadness. Mood-stabilizing medications for bipolar disorder differ from those used for other types of depression but can be quite helpful.
4. Seasonal affective disorder (SAD): The onset of this sort of sadness coincides with the shorter days of autumn and winter. Changes in the body’s natural daily rhythms, the eyes’ sensitivity to light, or the activity of chemical messengers such as serotonin and melatonin may cause mood shifts. The leading treatment is light therapy, which consists of daily sitting sessions in close proximity to a particularly bright light source. The conventional treatments for depression, such as psychotherapy and medication, may be useful as well.
Apart from these major four types of depression, the following also exist:
5. Reactive depression: If your doctor believes that adverse life events, such as a divorce or financial concerns, sparked your depression, they may classify it as reactive.
6. Cyclothymia: You may be diagnosed with cyclothymia if your moods are persistent and erratic. You may experience bouts of sadness and periods of euphoria, but these phases may not be sufficiently severe or prolonged to qualify as bipolar disorder.
7. Psychotic depression: If you encounter a severe episode of depression, you may get hallucinations or delusions. This condition is known as psychosis. A hallucination is the experience of hearing, seeing, smelling, tasting, or feeling things that are not real. A delusion is the tendency to believe things that are not true.
Depression types unique to women
Although women are more susceptible to general depression than males, they are particularly susceptible to two forms of depression driven by reproductive hormones: a) perinatal depression and b) premenstrual dysphoric disorder (PMDD).
a) Perinatal depression: This form of depression comprises both significant and small depressive episodes that occur during pregnancy or within the first year following delivery (also known as postpartum depression). Up to one in seven women who give birth experience perinatal depression, which can have catastrophic impacts on the women, their infants, and their families. The treatment consists of counseling and medication.
b) Premenstrual Dysphoric Disorder (PMDD): This form of depression is a severe manifestation of premenstrual syndrome (PMS). PMDD symptoms typically begin immediately after ovulation and subside when menstruation begins. Inhibitors of selective serotonin reuptake (SSRIs) such as fluoxetine (Prozac) and sertraline (Zoloft) may alleviate symptoms.
Unknown to many, pediatric depression also exists. Pediatric depression is a reasonably common psychiatric illness that frequently persists into adulthood.
DIAGNOSIS:
There are no scientific tests that specifically detect depression, but other probable causes such as an underlying disease must be checked and ruled out.
The following may be included in the workup:
i) Complete blood count with differential
ii) Serum electrolytes
iii) Blood urea nitrogen (BUN)
iv) Creatinine clearance and concentration
v) Urine osmolality
vi) Drug monitoring (if relevant)
vii) DSM-5: The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) published by the American Psychiatric Association may be used to diagnose depression.
The following further examinations may be necessary or helpful:
viii) Electroencephalographic recording (EEG)
ix) Electrocardiography (ECG)
x) Liver and Thyroid function tests
xi) Child Depression Inventory

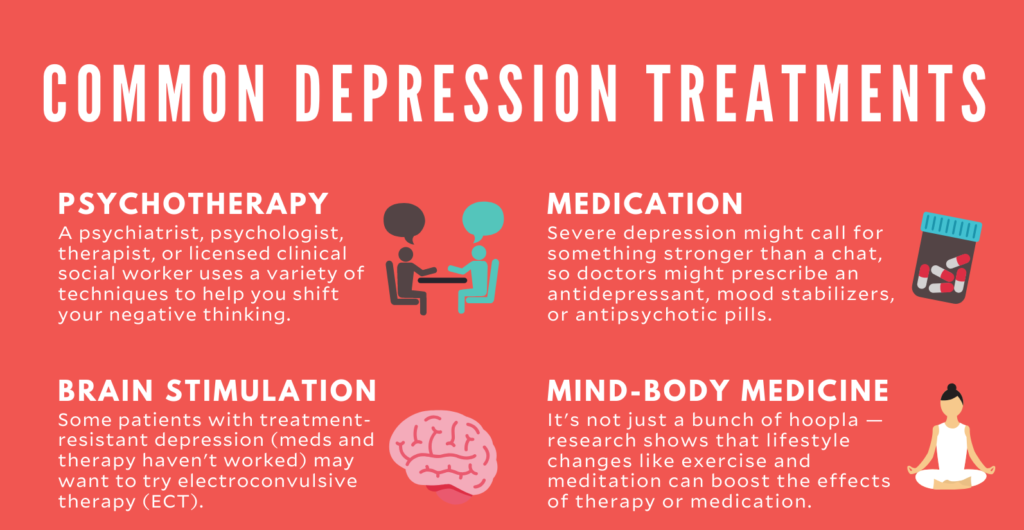
TREATMENT & MANAGEMENT:
Based on current research, children, adolescents, and adults with severe depressive illness should be treated with cognitive-behavioural therapy (CBT), medication, or a combination of the two. Safety is always the top priority while assessing depression. The risk evaluation of depressed patients should be continual. Clinical decision-making should be supported by documentation.
Multiple randomized clinical trials have demonstrated the efficacy of cognitive-behavioural therapy in the treatment of mild to moderate depression. Randomized clinical trials support the efficacy of 3 selective serotonin reuptake inhibitors (SSRIs): fluoxetine, sertraline, and citalopram, in the treatment of moderate to severe major depression.
There are numerous antidepressants available, including those I have listed below:
- Selective serotonin reuptake inhibitors (SSRIs); SSRIs are generally the first-line treatment prescribed by physicians. These antidepressants are considered safer and produce fewer adverse side effects than other types. SSRIs include citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), paroxetine (Paxil, Pexeva), sertraline (Zoloft), and vilazodone (Viibryd).
2. Serotonin-norepinephrine reuptake inhibitors (SNRIs); Examples of SNRIs include duloxetine (Cymbalta), venlafaxine (Effexor XR), desvenlafaxine (Pristiq, Khedezla), and levomilnacipran (Fetzima).
3. Atypical antidepressants; These antidepressants do not fit nicely into any of the other groups. They include bupropion (Wellbutrin XL, Wellbutrin SR, Aplenzin, Forfivo XL), mirtazapine (Remeron), nefazodone, trazodone and vortioxetine (Trintellix).
4. Tricyclic antidepressants.; These antidepressants, include imipramine (Tofranil), nortriptyline (Pamelor), amitriptyline, doxepin, trimipramine (Surmontil), desipramine (Norpramin), and protriptyline (Vivactil), can be quite helpful, but their adverse effects are typically more severe than those of newer antidepressants. Therefore, tricyclics are generally not prescribed unless an SSRI has been tried first without success.
5. Monoamine oxidase inhibitors (MAOIs); MAOIs, such as tranylcypromine (Parnate), phenelzine (Nardil), and isocarboxazid (Marplan), may be used when other medications have been ineffective due to their potentially severe side effects. MAOIs necessitate a rigorous diet due to severe (or even fatal) interactions with foods, medications, and herbal supplements, such as cheeses, pickles, and wines. Selegiline (Emsam), a newer MAOI applied as a patch, may be associated with fewer side effects than older MAOIs. These drugs are incompatible with SSRIs.
6. Other medications; Additional drugs may be combined with an antidepressant to increase its efficacy. Your doctor may suggest combining two antidepressants or adding mood stabilizers or antipsychotics. Short-term use of anti-anxiety and stimulant drugs may also be introduced.
Overall, the choice of initial acute therapy is determined by the following variables:
a. Severity
b. The number of previous occurrences
c. Chronicity
d. Subtype
e. Age of the individual
f. Contextual factors, such as family strife, academic difficulties, and exposure to adverse life events
g. Adherence to therapy
h. Previous treatment reaction
i. Patient and family motivation for treatment
Risks of abrupt medication withdrawal:
Do not stop taking your antidepressant without first consulting your doctor. Antidepressants are not thought to be addictive, but physical dependence (which is distinct from addiction) can sometimes develop.
Stopping therapy quickly or skipping multiple doses might result in withdrawal-like symptoms, and discontinuing abruptly can trigger a dramatic deterioration of depression. Work with your doctor to lower your dosage gradually and securely.
Antidepressants and pregnancy:
Some antidepressants may represent an increased health risk to your unborn or nursing kid if you are pregnant or breastfeeding. Consult your doctor if you become pregnant or want to become pregnant.

Antidepressants and increased likelihood of suicide:
It is required that all antidepressants must include a black box warning, the highest warning for prescriptions, despite the fact that the majority of antidepressants are generally safe. In some situations, children, adolescents, and young adults under the age of 25 using antidepressants may experience an increase in suicidal thoughts or behaviour, particularly during the first few weeks of treatment or when the dose is altered.
Those taking antidepressants should be constantly monitored for increasing depression or strange behaviour, particularly when beginning a new medicine or changing the dosage. If you or someone you know has suicidal thoughts while taking an antidepressant, seek help immediately.
Consider that antidepressants are more likely to minimize the risk of suicide in the long term by enhancing mood.
Other Treatment Options:
In moderate situations, psychosocial therapy is frequently recommended as first-line treatment, however, in severe cases, medication is frequently indicated in addition to psychotherapeutic intervention.
Depressed children and adolescents should be treated within a biopsychosocial setting. This method involves psychotherapies (e.g., individual, family, and group), medication management, social skills training, and educational evaluation and planning. Prior to initiating a treatment plan, the doctor must select an appropriate therapeutic environment.
Any doctor assessing a depressed person’s risk for suicide must do so with great care. If an individual is preoccupied with suicidal ideas, has clear intentions, or has other major suicide risk indicators, he or she must be hospitalized. When assessing whether or not one should be hospitalized, the clinician should consider aspects such as the person’s ability to function and the family’s stability, as well as any history of prior suicide attempts.
Other techniques, also dubbed brain stimulation therapies, may be recommended for some individuals:
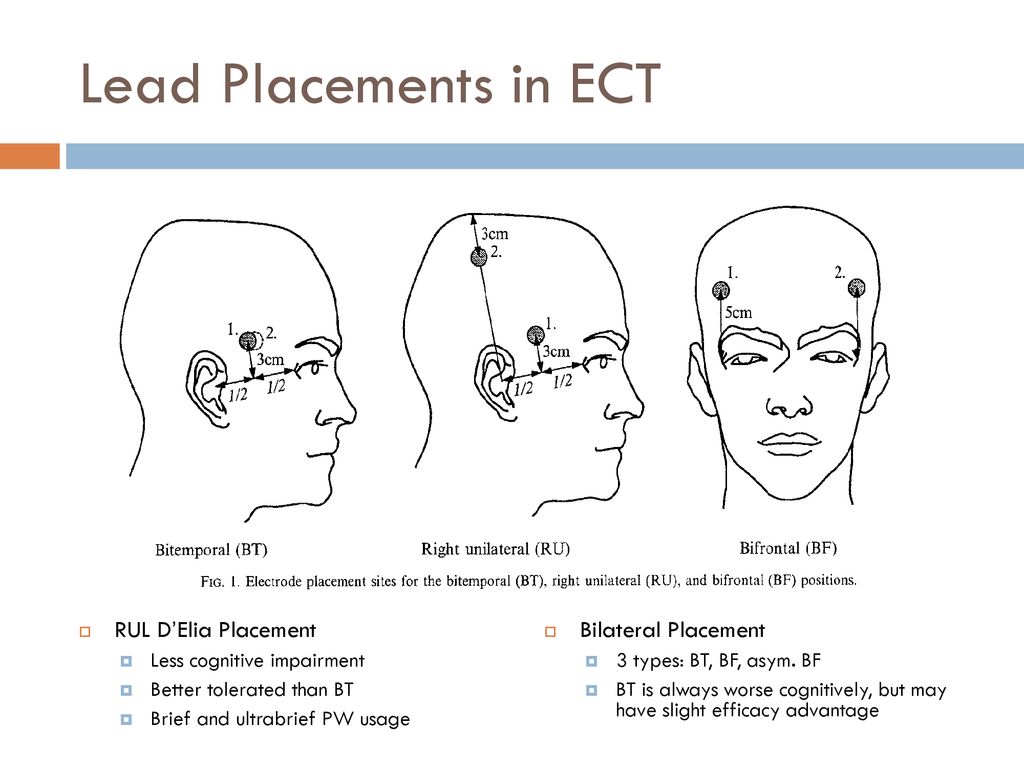
a. Electroshock treatment (ECT): In electroconvulsive therapy (ECT), electrical currents are sent through the brain to alter the function and action of neurotransmitters to alleviate depression. People who do not respond to medications, cannot take antidepressants for health reasons, or are at high risk for suicide are typically given ECT.
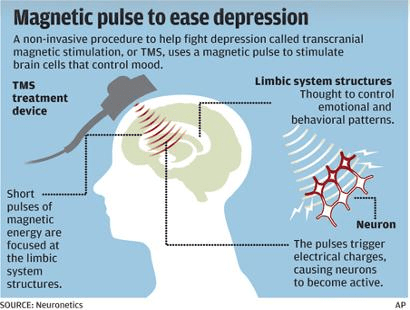
b. Transcranial magnetic stimulation (TMS): Those who have not responded to antidepressants may consider TMS. During transcranial magnetic stimulation (TMS), a treatment coil placed against the scalp emits short magnetic pulses to target nerve cells involved in mood regulation and depression.
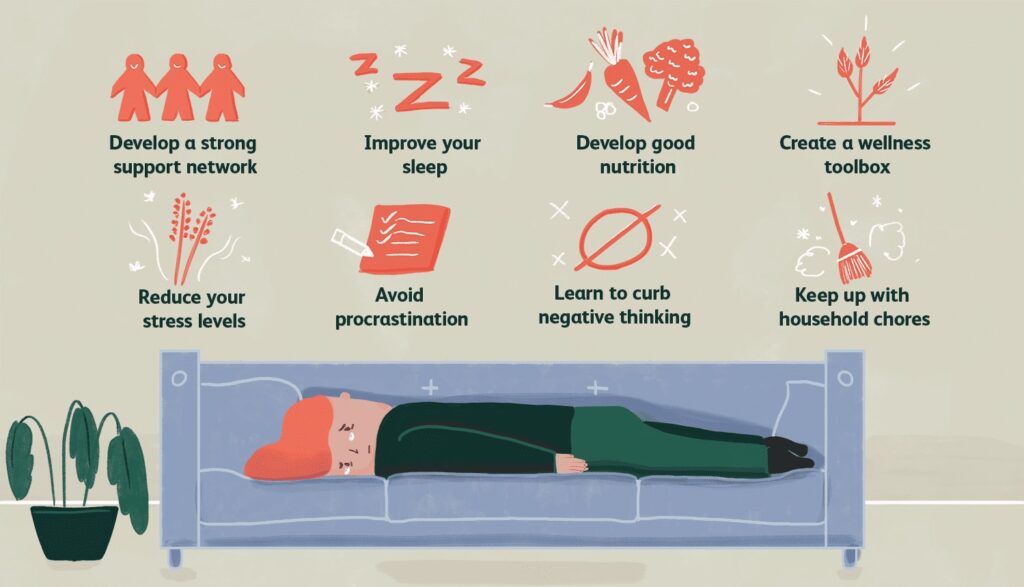
COPING & SUPPORT:
- Streamline your life; When feasible, reduce your obligations and create appropriate goals for yourself. Give yourself permission to do less when you feel depressed.
- Create a journal; As part of your treatment, writing in a journal may enhance your mood by allowing you to express pain, anger, fear, and other emotions.
- Consult authoritative self-help books and websites; Your doctor or therapist may recommend books or websites for you to read.
- Identify beneficial groups; Numerous organizations provide education, support groups, counseling, and other resources to assist those suffering from depression. Employee assistance programs and religious organizations may also provide assistance for mental health issues.
- Avoid being secluded; Regularly engage in social activities and get together with family and friends. Support groups for those with depression might help you connect with others facing similar obstacles and share your experiences.
- Learn methods of relaxation and stress management; Meditation, gradual muscular relaxation, yoga, and tai chi are among examples.
- Structure your time; Plan your day. Creating a list of daily chores, using post-it notes as reminders, or using a planner may help you keep organized.
- Don’t make important decisions when you’re feeling sad; When depressed, avoid making decisions because you may not be thinking clearly.
Phew, this was a long but necessary post in my opinion. I hope it will help someone out there currently battling depression. Know that you are loved, you matter, and that, this too shall come to pass.
Remember to take it one day at a time as Matthew 6 verses 25 -34 says;
Do Not Worry
“Therefore, I tell you, do not worry about your life, what you will eat or drink; or about your body, what you will wear. Is not life more than food, and the body more than clothes? Look at the birds of the air; they do not sow or reap or store away in barns, and yet your heavenly Father feeds them. Are you not much more valuable than they? Can any one of you by worrying add a single hour to your life?
“And why do you worry about clothes? See how the flowers of the field grow. They do not labor or spin. Yet I tell you that not even Solomon in all his splendor was dressed like one of these. If that is how God clothes the grass of the field, which is here today and tomorrow is thrown into the fire, will he not much more clothe you—you of little faith? So do not worry, saying, ‘What shall we eat?’ or ‘What shall we drink?’ or ‘What shall we wear?’ For the pagans run after all these things, and your heavenly Father knows that you need them. But seek first his kingdom and his righteousness, and all these things will be given to you as well. Therefore, do not worry about tomorrow, for tomorrow will worry about itself. Each day has enough trouble of its own.

Till next time. Winter is coming!
Leave a comment