
")
With the month of July slowly coming to an end, so is my focus on some of the most common female-related diseases. Our second from last post is dedicated to this benign, hormone-sensitive smooth muscle tumor of the uterus which is the most common tumor of the female genital tract, (sorry Dad if I got this last bit wrong).
The exact cause of uterine fibroids is unclear. Predisposing factors are;
- Nulliparity (having never carried a pregnancy beyond 20 weeks of gestation (point of viability)).
- Early menarche (onset of Aunt Flo) below the age of 10
- Age 25-45 (they are largely found in women of reproductive age)
- Increased incidence in African (black women have a higher incidence of leiomyomas, more symptomatic fibroids, earlier presentation, and increased severity of disease)
- Obesity
- Family history

They are influenced by hormones (i.e. estrogen, progesterone, and the growth hormone). During menopause, there is a decrease in hormone levels which directly results in the shrinking of leiomyomas.
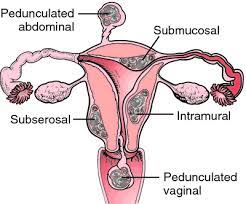
Leiomyomas commonly known as fibroids are classified according to their location within the uterus:
- Subserosal leiomyoma: localized in the outer uterine wall beneath the peritoneal surface. These may be sessile or pedunculated and grow out of the uterine wall. Subserosal fibroids may also attach themselves to neighbouring adjacent abdominal structures such as the bowel.
- Intramural leiomyoma: this is the most common type and it grows from within the wall of the myometrium (the smooth muscle layer of the uterus wall between the inner uterine layer (endometrium) and the outer uterine layer (serosa). By definition, these do not distort the endometrial cavity.
- Submucosal / subendometrial leiomyoma: localized directly below the uterine mucosa (endometrial layer). These can be further subdivided into 3 types: Type 0, pedunculated (attached to the submucosal endometrial layer by a narrow stalk), fibroids without any intramural extension. These may protrude through the os of the cervix and undergo torsion and infarction. Type I, sessile with less than 50% intramural extension.
Type II, sessile with more than 50% intramural extension.
4. Diffuse uterine leiomyomatosis: here, the uterus becomes grossly enlarged because of the presence of numerous fibroids. The symptoms vary and depend on the leiomyoma locations.
A major limitation of the classification is that it doesn’t take into account the size of the fibroids. Based on this classification, any fibroid larger than 4cm that does not distort the uterine cavity would be classified as subserosal, even though it might be present in the entire thickness of the myometrium (normal thickness is 15-20mm).
It is a truth universally known that most women dream of becoming mothers someday for different reasons. Some so they can have someone to order about like how our mothers order us about, some so they can have a pregnancy photo shoot, and some because the Bible says, ‘’go forth and multiple”. So, let us now take a look at:
I. Effects of myomas on pregnancy.
II. Effects of pregnancy on myomas.
I. These common tumors are associated with a number of obstetrical complications such as excessive preterm labor, placental abruption, fetal malpresentation (breech, shoulder, face, and brow), obstructed labor, cesarean delivery, and postpartum hemorrhage. A study conducted in 2065 women with leiomyoma reported that; Placental abruption and breech presentation increased fourfold, first-trimester bleeding and dysfunctional labor increased twofold, and cesarean delivery increased sixfold. Another study showed reported an eightfold second-trimester abortion risk.
The two most important factors in determining morbidity are the size and location of the myoma. Closeness to the placental implantation site is important. Abortion, placental abruption, preterm labor, and postpartum hemorrhage all are increased if the placenta is adjacent to or implanted over a fibroid.
Myomas in the cervix or lower uterine segment are particularly troublesome because they are most likely to cause an obstruction of labor. Larger myomas distort anatomy and push the uterus laterally, this most likely leads to a complete inferior vena caval obstruction making hemorrhaging more likely at cesarean delivery and a hysterectomy (operation to remove the uterus) can be technically difficult. In some cases, fibroids that are adjacent to the birth canal may be carried upward as the uterus becomes larger.
The recommended management of myomas during pregnancy after the diagnosis has been confirmed is expectant management.
II. The stimulatory effects of pregnancy on the growth of uterine fibroids may be somewhat impressive. I could go all full science nerd but I will just summarise it. In pregnancy the estrogen receptors are suppressed, therefore fibroid growth in early pregnancy is stimulated by similar hormonal and growth factors that cause normal uterine growth.
However, myomas respond differently in individual women so an accurate prediction of their growth is not possible.
What are the clinical features? Well, most women have small, asymptomatic fibroids. Symptoms depend on the number, size, and location of leiomyomas. Abdominal pain, anemia, and increased bleeding can be indicative of uterine fibroids.
- Abnormal menstruation:
-hypermenorrhea
-menorrhagia
-metrorrhagia (anemia associated)
-dysmenorrhea
2. Features of mass effect:
-enlarged, firm, and irregular uterus
-back or pelvic discomfort or pain (labor-like pain if the leiomyoma is within the cervical os)
-urinary tract or bowel symptoms (urinary retention/ frequency, constipation)
-abdomen can grow larger (mimicking the appearance of pregnancy)
3. Reproductive abnormalities:
-infertility (increased risk of miscarriage and difficulty conceiving)
-dyspareunia (anterior or fundal fibroids often cause severe pain during sex)

In some rare cases, large fibroids can extend out through the cervix and vagina.
Fibroids can be mistaken for ovarian neoplasms such as Sarcoma botryoides (more common in children and adolescents). Palpation during a pelvic examination can identify larger fibroids, for a confirmed diagnosis, 2 main imaging modalities are used;
- Transvaginal ultrasonography (best initial test)
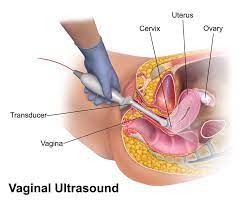
- Hysterosalpingography (HSG)

MRI is mainly used in cases where the evaluation of the uterus and ovaries has to be done for potentially complicated surgical cases and visually differentiate between leiomyomas, adenomyomas, and adenomyosis.
When it comes to treatment the 2 questions that have to be addressed are: which fibroids should be treated, and how should they be treated?
Treatment should only be considered in symptomatic patients because of the side effects associated with medical therapy and surgery.
Medical therapy:
i) Hormone therapy:
- Gonadotropin-releasing hormone (GnRH) agonist such as LEUPROLIDE, GOSERELIN, NAFARELIN. These work by causing a “medical menopause” leading to reduction in estrogen which leads to a decrease in size of leiomyomas. They are the optimal treatment before surgery but should not be used for more than 6 months. Leiomyomas grow back once therapy is discontinued.
- Combined oral contraceptive pill & progestin-only contraceptive pill. These control bleeding and pain but may promote the growth of leiomyomas. They are usually combined with GnRH agonist (dual therapy).
- Progestin-releasing intrauterine device (IUD): it does not treat fibroids but rather controls heavy and painful bleeding. It is used only for fibroids that do not distort the inside of the uterus.
ii) Antifibrinolytics such as TRANEXAMIC ACID. These reduce heavy bleeding.
iii) Androgenic agonists such as DANAZOL. They suppress the growth of fibroids but have a lot of side effects such as hair loss, acne, and, edema.
iv) NSAIDs (nonsteroidal anti-inflammatory drugs). They are used for dysmenorrhea.
Interventional therapy:
i) Uterine fibroid embolization: uterine artery embolization (UAE). Indications for this are; continued heavy bleeding and/ or severe pain with insufficient response to medical treatment, contraindications to surgery or personal preference to avoid surgery, and lack of interest to conceive in the future. The procedure is done by injecting polyvinyl alcohol (PVA) into the arteries that supply blood to the fibroid, causing it to reduce in size.

NB; FURTHER INVASIVE TREATMENT IS REQUIRED IN 25% OF PATIENTS.
ii) MRI-guided focused ultrasound: in this procedure, energy from multiple elements of a phased array transducer is directed through the anterior abdominal wall resulting in coagulative necrosis of the fibroid where the ultrasound waves converge. A 24-month follow-up study showed that this management option resulted in sustained relief of fibroid symptoms.
NB; CONSIDERING THAT NEITHER THE OVARIAN NOR THE ENDOMETRIAL BLOOD SUPPLY SHOULD BE AFFECTED DURING THIS PROCEDURE, THE METHOD MAY PROVE PROMISING FOR WOMEN WHO SEEK FERTILITY TREATMENT.
Surgical therapy:
Indications for surgical therapy are; rapidly growing fibroid, recurrent refractory bleeding secondary to medical therapy, and severe symptoms.
i) Myomectomy has long been regarded as the standard treatment for the various symptoms associated with fibroids, such as pelvic pressure, pain, or menorrhagia. In most cases, this is the best option for women who are interested in preserving their fertility. Submucosal, intracavitary, and in some cases intramural fibroids should be treated.
ii) Hysterectomy: definitive treatment.

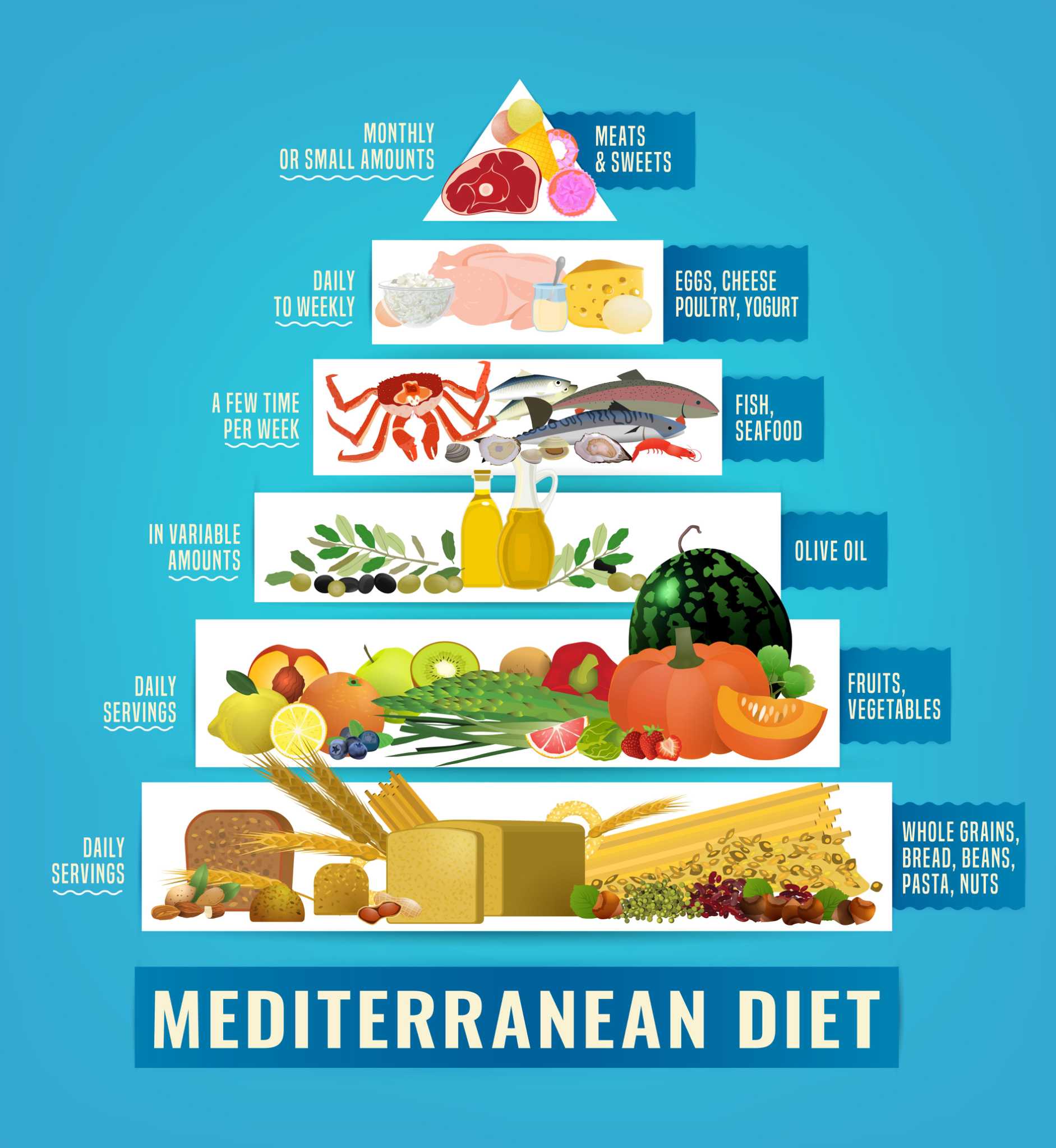
There are some diet and lifestyle changes one can make that might help reduce your risk for fibroids:
- Follow a Mediterranean diet. Add plenty of fresh and cooked green vegetables, fresh fruit, legumes, and fish to your plate.
- Cut back on alcohol
- Balance estrogen
- Lose weight if you are obese
- Avoid hormone-disrupting chemicals such as fertilizers, pesticides, dyes, paints.
- Lower your blood pressure by avoiding adding salt, limit high-sodium processed and packaged foods.
- Get enough vitamin D by eating egg yolks, milk, cheese.
Diet alone can’t treat fibroids, but, a balanced diet may also help ease some fibroid symptoms and complications.
Below you will find a list of foods to eat if you have fibroids;
- Fibre-rich foods (vegetables, fruit, whole-grain bread and pasta, oats, barley, beans)
- Potassium (avocado, bananas, citrus, lentils, potatoes, tomatoes)
- Dairy (yoghurt, full-fat cheese)
- Green tea
Foods to avoid if you have fibroids:
- Sugar (table sugar, glucose, corn syrup, white bread, rice, pasta, and flour, soda and sugary drinks, fruit juice, potato chips, packaged energy bars
- Estrogen-increasing foods (red meat, soy beans, soy milk, tofu, flax seed)
- Takeaway
Phewwww, this was a long read for you, and write for me.
Here’s to hoping you all found it enlightening.
STAY SAFE & SEE YOU SOON!
Leave a comment